Tens of thousands of Czech people protested October 28, demanding the current government resign and sanctions against Russia end / credit: Screenshot from video
Editor’s Note: This article originally appeared on Antiwar.com.
Amid ever escalating tensions over the West’s proxy war in Ukraine and the devastating inflation ripping Europe apart, Czech protesters gathered October 28 in Prague demanding the coalition government’s resignation, the Associated Press reports.
The rally saw tens of thousands of citizens condemning their government’s support for Kiev, including the provision of heavy weapons, as well as sanctions on Russia. A smaller, similar rally was held in Brno, the country’s second-largest city.
The demonstrators’ slogan was “Czech Republic First.” As with other recent protests throughout the continent, the left and right are uniting in their opposition to the West’s economic and proxy warfare against Russia.
One speaker said “Russia’s not our enemy, the government of warmongers is the enemy,” according to the AP.
Protesters “repeatedly condemned the government for its support of Ukraine and the European Union sanctions against Russia, opposed Czech membership in the EU, NATO and other international organizations,” the report said.
Leaders in Prague dismissed the protests. Interior Minister Vit Rakusan tweeted “[w]e know who’s our friend and who’s bleeding for our freedom,” adding “we also know who’s our enemy.”
The Washington-led sanctions blitz has cut Europe off from cheap Russian gas upon which it has long relied. In the Czech Republic, energy, housing, and food prices soaring. The inflation rate is 17.8 percent.
Similar protests are occurring in Italy, Germany, and France. “Strikes and protests over the rising cost of living proliferate, ushering in a period of social and labor unrest not seen since at least the 1970s,” the New York Times reported earlier this month.
In September, Prague saw massive demonstrations of 70,000 people, again from the left and right, protesting against NATO’s proxy war in Ukraine and rising energy prices caused by the sanctions campaign. Those protesters also called for the resignation of Prime Minister Petr Fiala’s center-right coalition government. “We intensively support the justified fight of the Ukrainian people,” Fiala has declared.
Wow. Absolutely massive protest in Prague, Czech Republic today demanding an end to anti-Russia sanctions. pic.twitter.com/GtjHWdEhl4
Connor Freeman is the assistant editor and a writer at the Libertarian Institute, primarily covering foreign policy. He is a co-host on the “Conflicts of Interest” podcast. His writing has been featured in media outlets such as Antiwar.com, Counterpunch, and the Ron Paul Institute for Peace and Prosperity. He has also appeared on “Liberty Weekly,” “Around the Empire” and “Parallax Views.” You can follow him on Twitter at @FreemansMind96.
South Africa wants peace between Ukraine and Russia. That was the message from the head of the country’s ruling ANC party, during a feisty interview with the BBC. Fikile Mbalula also stressed his party would welcome the Russian President if he attended the… pic.twitter.com/prUckb7xI6
South Africa wants peace between Ukraine and Russia. That was the message from the head of the country’s ruling African National Congress (ANC) party during a contentious interview with the British Broadcasting Corporation (BBC). Fikile Mbalula also stressed his party would welcome Russian President Vladimir Putin if he attended the upcoming BRICS (Brazil, Russia, India, China, South Africa) summit in Durban, South Africa. That’s despite the International Criminal Court issuing an arrest warrant for Putin over alleged war crimes in Ukraine. Digital news outlet African Stream breaks it down.
A U.S. Air Force Douglas Skyraider drops a white phosphorus bomb on a Viet Cong position in South Vietnam in 1966 / credit: U.S. Air Force
Editor’s Note: The following is the writer’s opinion.
“More of us took our own lives after returning home than died in the battle.” -statement of U.S. armed forces veterans on U.S. war on Vietnam
In the analysis of all exploitative systems, it is obvious to see how the exploited are harmed. This is where most attention has been focused, and understandably so.
Nevertheless, it is also important to examine and understand what happens to the exploiters at the other end of the process of exploitation.
The reason is, invariably, in any process of exploitation, exploiters are also harmed in ways that are serious and significant, even though they may be less visible and obvious immediately. This is partly the reason why this aspect of exploitation is less recognized. If there is a better understanding and a wider recognition of how exploiters suffer in the process of exploitation, new openings can emerge to convince the more powerful regarding the futility of prolonging exploitative relations and systems.
For the sake of brevity, here we speak mostly in terms of only two ends of exploitation systems—the exploiters and the exploited. But we also can speak of two ends of systems of dominance—the dominators and the dominated. Or the two ends of systems of conquest—the conqueror and the conquered.
One indication of what happens to the exploiter or the conqueror is available in some statements of the veterans of U.S. armed forces. One of these statements, which described the immense cruelties and killings, said, “We know what Post Traumatic Stress Disorder looks like, feels like and tastes like because the ghosts of over 2 million men, women and children still haunt our dreams. More of us took our own lives after returning home than died in battle.”
A detailed account followed the life of a pilot whose napalm bombing had led to the burning of a Vietnamese girl, Kim Phuc. After returning home, this pilot kept looking at the picture of Kim in flames. This girl was roughly the same age as his son. “He could almost smell the child’s burning flesh.” The veteran had nightmares of screaming children pointing accusing fingers toward him. There was a breakdown in his family. He turned to alcohol. “He drank to put the bombing out of his mind, and the drinking made him more obsessed.”(Reader’s Digest, November 1997).
This is by no means an isolated case. Breakdowns in close relationships, substance abuse, domestic violence, self-violence and suicide attempts have been found to be very high among soldiers who return home after fighting highly unjust wars. More commonly, anyone who performs unjust and exploitative actions over a period of time is likely to be able to continue this only by giving up on the sensitivity needed for care, compassion and love. Hence, this person’s ability to fulfill close relationships based on this declines steadily, as also his ability to experience those forms of happiness associated with real love, caring relationships and compassion.
At a wider level, a group or society which seeks to enrich itself by plundering and exploiting others has to spread value systems that make their members insensitive to the sufferings of others. But in the process of making them insensitive, the foundation also is prepared for breakdown of internal social relations (including with the closest people), internal violence, self-violence and falsehoods. This can be seen in exploiter and conqueror societies as well as at individual levels, in the hollow lives of those who lead aggressions.
To give one example of such impacts, the example of Christopher Columbus may be cited. The extreme cruelties driven by the endless greed of this explorer are well-known. What kind of personality this turned him into is best revealed by a reputed doctor, Sigmundo Feliz, who attended to him in his final years:
“To be without roots, without a sense of home and place is one of the most serious, though one of the least emphasized, psychological disorders. This patient suffered from this to an unusual degree… This patient appears from all evidence to be someone who found it difficult, even in non-threatening circumstances, to tell the truth, a habit of delusion that at times turned into self-delusion.”
At the level of entire societies, those which lead by aggression toward others, culminating in wars, are often engaged in spreading falsehoods and self-delusions, media and education systems being two commonly used channels. The big lies cooked up to justify aggression for plunder or domination get transferred also to almost equally big lies cooked up to justify internal exploitation by big business interests. Hence, people are exposed to serious health hazards by big business interests; in some cases the toll in the longer term may be higher than that of even destructive wars. Therefore, not just at the level of individuals but also at the level of entire societies, exploiters also suffer in serious ways.
The aggression and weaponization abroad is also reflected in internal violence. The United States, for example, experienced:
1.2 million recorded violent incidents in 2019 (366 per 100,000 people), according to FBI data;
Over 10 million arrests this year (not counting traffic violations), which comes out to 3,011 arrests for every 100,000 people;
The highest number of prisoners per capita in the world;
Seven people dying a violent death every hour; and
19,100 homicides and 47,500 suicides in 2019.
According to official U.S. data, this year 12 million people seriously thought about suicide, while 3.5 million planned a suicide attempt and 1.4 million attempted suicide.
Among U.S. youth, suicide is the second highest cause of death. Plus, an unprecedented increasing trend of suicide attempts have been reported among U.S. youth during the last decade, and more pronounced among girls.
Some of this data points to a deep internal social crisis that can arise within an exploiter-and-conqueror society known for its invasion and aggression. Careful research is likely to reveal more links of aggression and internal distress. Such research should be used to convince more people about the futility of paths based on exploitation, dominance and conquest.
Bharat Dogra is Honorary Convener, Campaign to Save Earth Now. His recent books include Planet in Peril and Earth Beyond Boundaries.
More than 3,000 Accredited Social Health Activists (ASHAs) protested in the city of Kolhapur in India’s Maharashtra state on October 26 after several of their demands, such as the legal status of full-time workers, better working conditions, adequate pay, medical insurance, and others, weren’t met / credit: Sanket Jain
Prajakta Khade walked into a public health center daily for three months in early 2021, without ever receiving medical care. The healthcare worker’s 26 notebooks—containing more than 3,000 pages of community health records—point to why she couldn’t seek treatment for her ailments. She was simply too busy.
In March 2020, India’s health ministry tasked 1 million Accredited Social Health Activists (ASHAs) like Khade with COVID-19 duty in rural areas. This, in a country where 65 percent of its 1.38 billion people live outside cities. Suddenly, ASHAs’ workload increased exponentially. Yet, they remain underpaid and now suffer stress-related chronic ailments.
“If a positive case was found in the area, we had to visit the patient, contact trace, arrange medical facilities, measure their oxygen and temperature levels daily, and ensure they complete quarantine,” Khade explained about the added duties to treat the infectious respiratory disease. But all Khade was given to do her job in the assigned area in India’s Maharashtra state was a single N95 mask and 200 milliliters of sanitizer.
ASHAs, an all-women healthcare cadre, remain the foot soldiers of India’s rural healthcare. One worker is appointed for every 1,000 citizens under India’s 2005 National Rural Health Mission. ASHAs are responsible for more than 70 tasks, including providing first-contact healthcare, counsel regarding birth preparedness, and pre- and post-natal care. Plus, they help the population access public healthcare and ensure universal immunization, among other things.
The World Health Organization announced a pandemic in March 2020. But in many countries, lack of adequate healthcare and no social safety nets amid lockdowns wrecked the lives of ordinary people. In India, for example, an additional 150 million to 199 million people are expected to enter poverty in 2021 and 2022.
Chronic Illnesses Spike
One day about a year ago, while surveying people in her village of Vhannur in India’s Maharashtra state, 40-year-old Khade felt dizzy. But she couldn’t take a break. “At one point, my face was swollen, and I could barely see anything.” It turned out her blood pressure level had surged to 252/180 mmHg (millimeter of Mercury), much higher than the standard limit of 120/80. That is how she got diagnosed with hypertension.
However, a month’s worth of medications didn’t help because she continued to experience stress as her workload increased. Senior officials at the health center had early on issued an order to submit patient records daily by noon.
ASHAs, who aren’t considered full-time workers, receive performance-based incentives paid on the number of tasks completed. “For COVID duty, the government decided our worth as merely 33 Indian Rupees per day (43 U.S. cents),” she said. “We received this amount only for three months in the past two years.”
Moreover, during the peak of COVID-19 cases in 2021, salaries for Maharashtra’s ASHAs were delayed by five months, according to Khade. Netradipa Patil, an ASHA from Maharashtra’s Kolhapur district and leader of a union that represents more than 3,000 ASHAs, confirmed this.
One day last year, Khade’s supervisor asked for a list of hypertension and diabetes patients from her village of about 1,200 people—at 10 o’clock at night.
“How could I survey the entire community in the night?” she asked.
Often, such orders meant skipping lunch and staying hungry for 11 hours at a stretch. ASHAs worked four hours prior to the pandemic. Now, 12-hour days are normal.
When medications didn’t help, Khade consulted two private doctors. “After six months of hassle, the doctor doubled my dose to 50 milligrams.” Khade lost over 10 kilograms (22 pounds) of weight and was placed on medications to address anxiety. Even today, she suffers from fatigue.
“I was never this weak,” she asserted.
Chronic diseases among ASHAs are rising rapidly because of the workload, says Patil. “We protect the entire community, but there’s no one to look after our health.” ASHAs in Maharashtra, she says, average a monthly income of Rs 3,500 to 5,000 ($45 to $66 USD).
This reporter spoke to ASHAs’ senior officials from Maharashtra’s Kagal block. (In India, a cluster of villages form a block and several blocks form a district. Vhannur village is in the Kagal block of Maharashtra’s Kolhapur district.) Senior officials said they are not responsible for ASHAs’ deteriorating mental and physical health, and pointed to the Indian government’s order to submit data. The officials didn’t want to be named. Instead, they relayed that they also are overworked.
“ASHAs do the majority of the health department’s work, and they are massively underpaid for their duty,” said Dr. Jessica Andrews, a medical officer at Kolhapur’s Shiroli Primary Health Center. She has been handling mental health cases. “Without them, the health system will collapse.”
‘Not Treated As Humans’
Several ASHAs across India have worked for over a year without a break. One of them is Pushpavati Sutar, 46, diagnosed with hypotension (low blood pressure) and diabetes within seven months of COVID-19 duty in November 2020. Like Khade, she experienced constant spells of dizziness.
“Often, there was fake news of community COVID transmission in my area,” she said.
Every day, senior officials at the health center hounded her to find more details about such instances.
An ASHA for 13 years, she’s never made an error in her surveys and was sure of no community transmission. “After investigating, I found that the accused was COVID negative. Instead, two of his relatives were positive.”
She had to clear such misconceptions almost every day, answer senior officials’ questions, collect records and perform her regular duty. “For several days, I couldn’t sleep,” she remembered.
Further, fearing COVID-19 guidelines and quarantine rules, community members began demanding ASHAs hide COVID-19 cases. “People even accused us of spreading COVID as we would survey the entire village,” Sutar recounted. Moreover, she said senior officials asked ASHAs to visit the families of COVID-19 patients—instead of allowing data collection over the phone—putting them at risk of infection.
“At several places, there have been instances of community violence, where ASHAs were beaten up,” said Patil, who has filed legal complaints on behalf of the assaulted workers and is helping them mentally recover.
Kolhapur’s ASHA union has written to several government authorities, including Maharashtra’s chief minister and Indian Prime Minister Narendra Modi, highlighting the mental toll of COVID-19 duty. Still, none of their letters have garnered a helpful response.
“Forget adequate pay,” said Khade, as she continued surveying, juggling between completing her task and trying to keep her mind at ease. “We are not even treated as humans.”
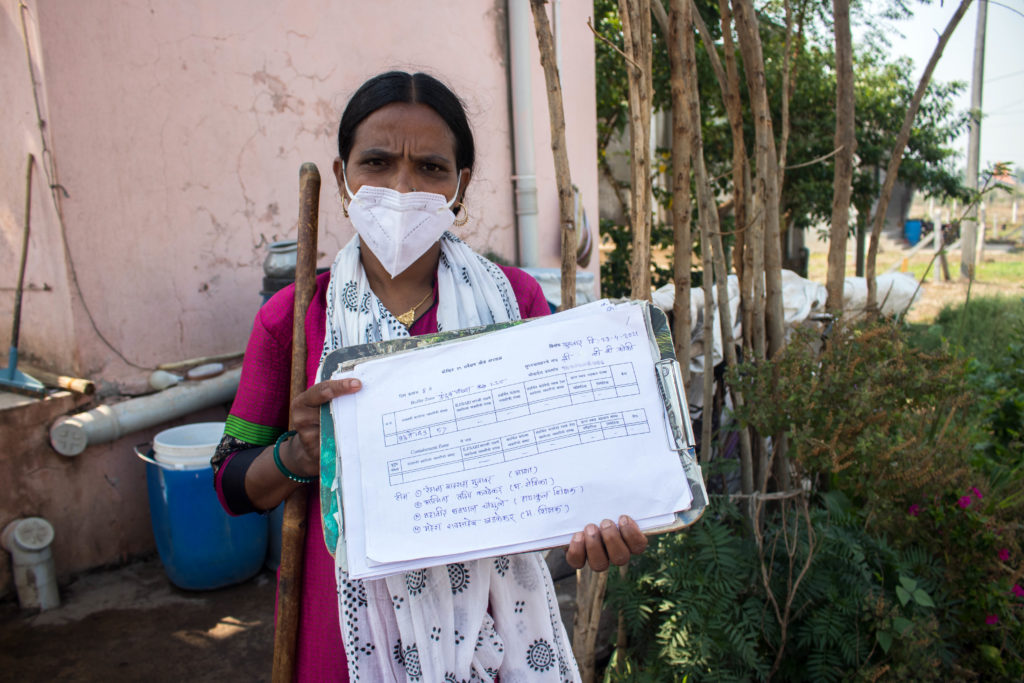
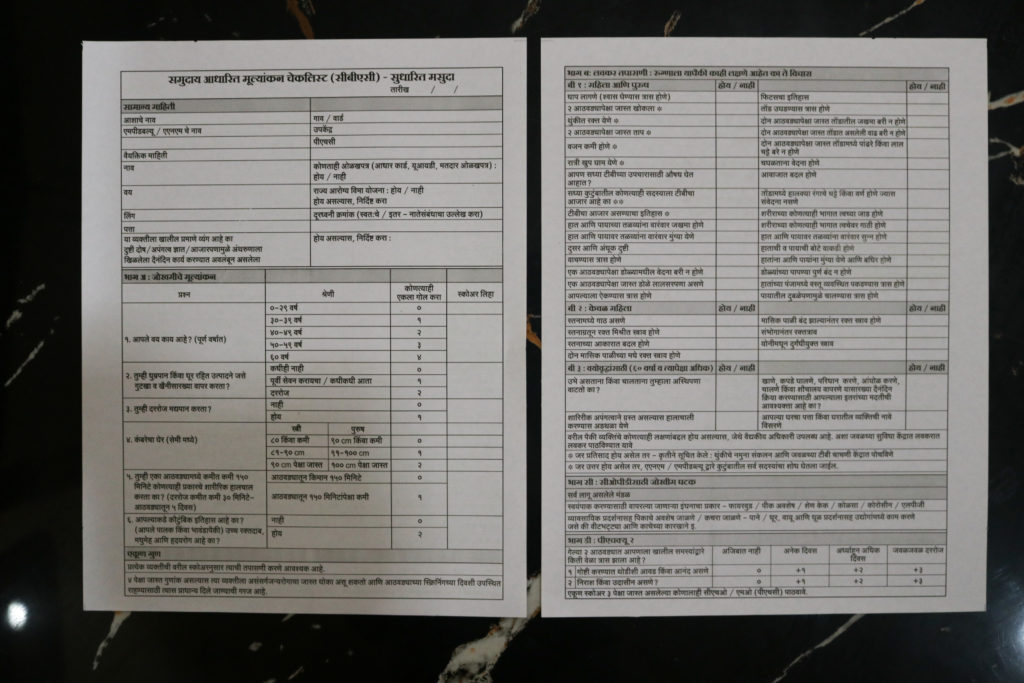
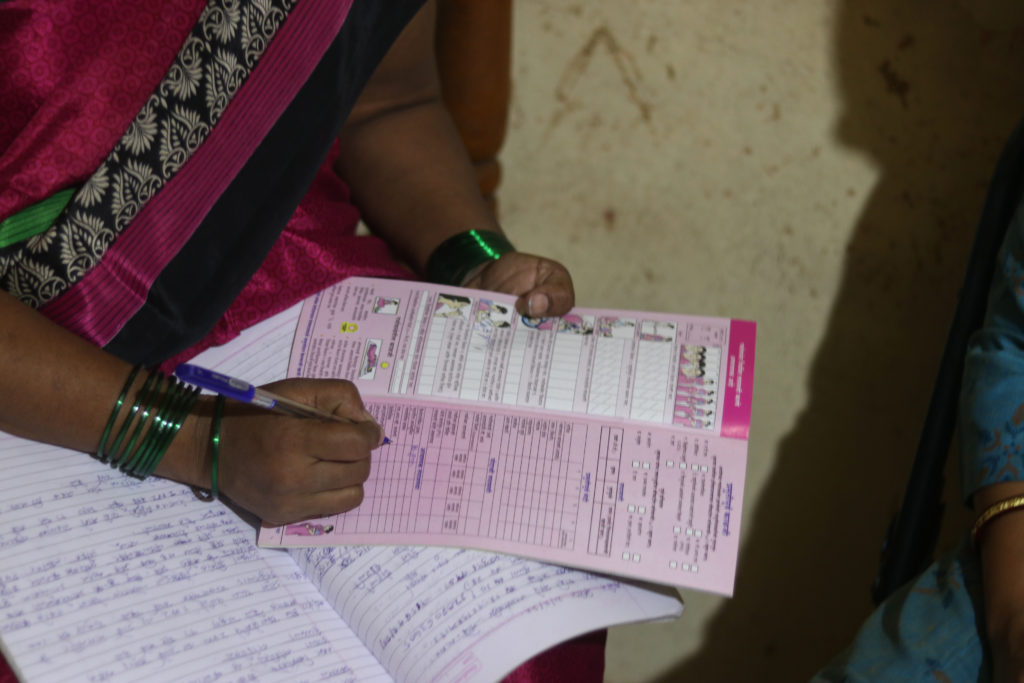
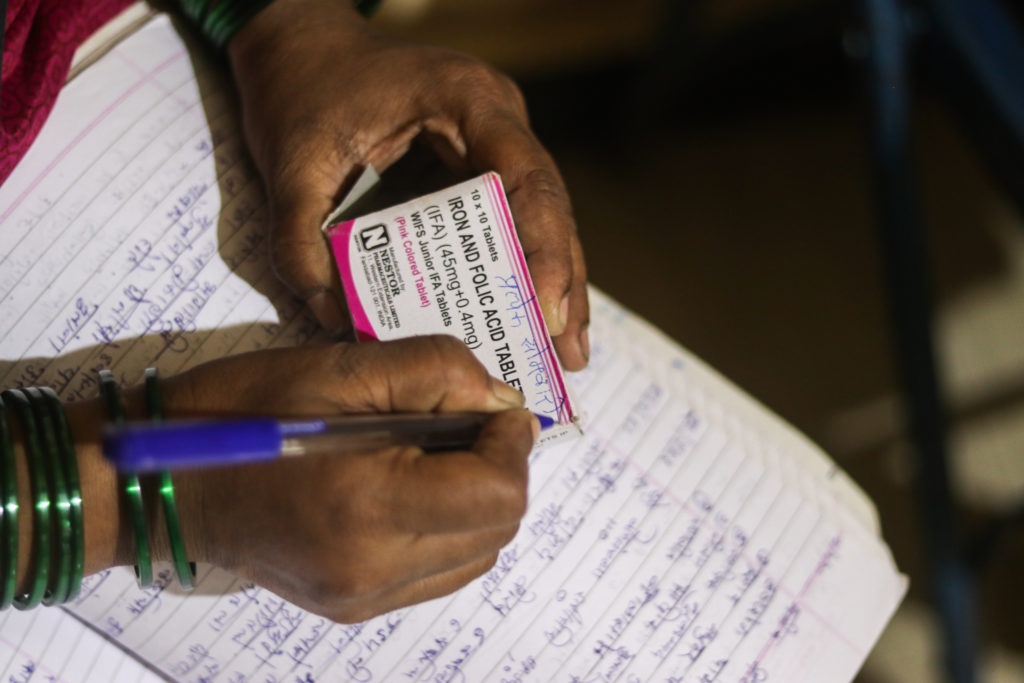
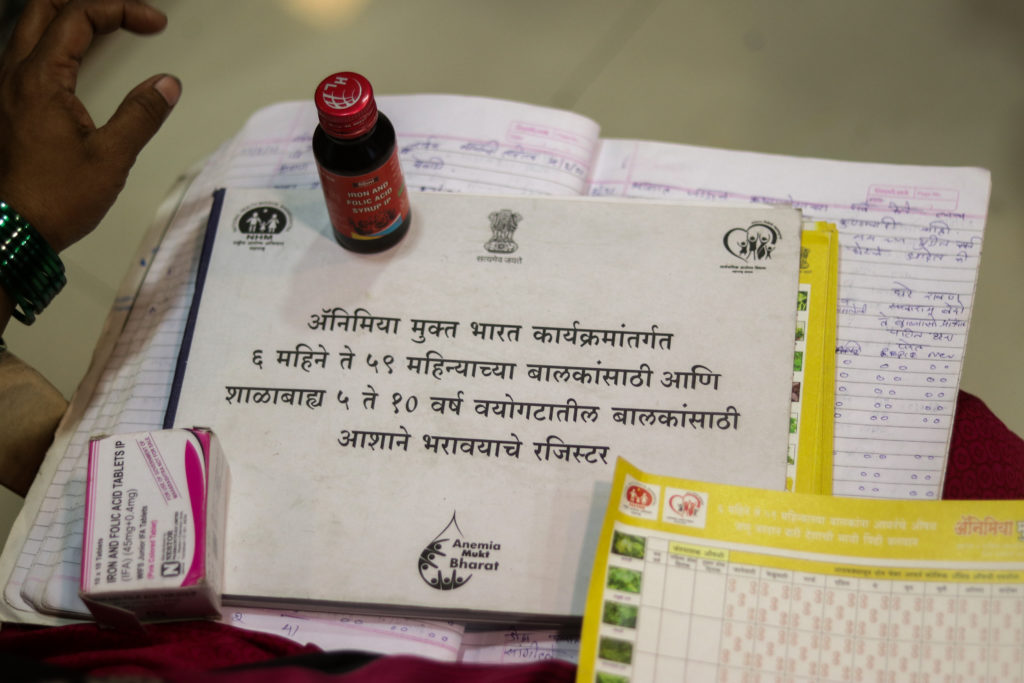
ASHA Rehana Mujawar, of Maharashtra’s Tardal village, shows COVID-19 records she is required to fill out every day by visiting her community of more than 1,000 members / credit: Sanket JainASHA workers Rekha Dorugade and Mandakini Kodak trekking the Dhangarwada hill to complete their survey, a steep patch of 5 kilometers (3.1 miles) in Kolhapur’s Pernoli village / credit: Sanket JainAn ASHA worker took a selfie as part of their protest on July 21 in Maharashtra’s Kolhapur city / credit: Sanket JainASHA workers protest outside the district collector’s office in Kolhapur city with placards mentioning their workload. In the center, wearing a red saree, is ASHA union leader Netradipa Patil, who has been fighting for better working conditions for over a decade / credit: Sanket JainASHAs across India have been protesting for better pay, full-time worker status and proper working conditions / credit: Sanket JainIndia has 810 district hospitals for 833 million rural people. In mountainous regions like Kolhapur’s Masai Pathar, ASHAs often trek, risking their lives to save pregnant women and make healthcare facilities accessible / credit: Sanket JainAn ASHA worker explains breastfeeding and taking care of a newborn to a community woman in Maharashtra’s Khutwad village / credit: Sanket JainIn Kolhapur’s Khutwad village, ASHA Maya Patil informs a migrant sugarcane cutter, whose relative gave birth to a child a month prior, about post-natal care and how they can access public healthcare facilities / credit: Sanket JainTo inspire fellow ASHAs, Netradipa Patil shares a WhatsApp status quoting lyricist and poet Gulzar: “Milta To Bahut Kuch Hai Is Zindagi Me, Bas Ham Ginti Usi Ki Karte Hain, Jo Hasil Na Ho Saka. (We get many things in life, but we only count the things we couldn’t achieve) / credit: Sanket JainASHAs also distribute iron, calcium, and vitamin tablets, among others, to community women and children every month. “For distributing these medicines, we’re merely paid Rs 100 ($1.30 USD),” says ASHA Netradipa Patil / credit: Sanket JainASHA Prajakta Khade collected the sputum of a patient she suspects to be a tuberculosis patient / credit: Sanket Jain“Be it any health record, the health department relies on our surveys and fieldwork,” says Khade, who has been an ASHA since 2009 / credit: Sanket JainWomen often share their health and mental issues with ASHA workers, as they have built a safe bond over the past decade / credit: Sanket JainAs part of the Health Ministry’s program of reducing non-communicable diseases, ASHAs across Maharashtra are tasked with surveying communities by asking them more than 60 questions. “We will merely be paid Rs 5 (6 U.S. cents) per form for collecting and filling in all the details,” says Khade / credit: Sanket JainA significant part of Khade’s time goes into filling out by hand medical records. “If any record is incomplete, our seniors immediately probe an inquiry, and even the pay is deducted,” she says / credit: Sanket JainSo far, Khade has spent over Rs 10000 ($131 USD) on doctors, medical tests, and medications, an equivalent of three months of her salary. “ASHAs don’t receive any health support system from the government, nor any medical insurance,” she says / credit: Sanket JainASHA Jayashree Khade from Kolhapur’s Vhannur village tested positive for COVID-19 in May 2021. “None of my seniors even once asked about my health. It was only the fellow ASHAs who helped me,” she says / credit: Sanket JainPrajakta Khade gives a plastic bottle to a community woman asking her to submit sputum for tuberculosis detection / credit: Sanket JainPushpavati Sutar, as part of postnatal visits, often counsels women on breastfeeding, seeks regular updates on the health of both the mother and the newborn, and provides the required medications / credit: Sanket JainAn ASHA worker filling out health records of a newborn in Kolhapur’s Shirol region, noting important details / credit: Sanket JainSutar distributes iron and folic acid tablets to her community members / credit: Sanket JainTo ensure community members take medications and supplements on a schedule, ASHAs often write instructions in the native language on the box / credit: Sanket JainSutar ignored her hypotension symptoms for several months and continued the survey because of the tremendous workload / credit: Sanket JainASHA workers always counsel community members on proper healthcare. Here, she is talking to a woman in Kolhapur’s Shirol region about early childhood health / credit: Sanket JainAs part of the health ministry’s Anemia Free India program, ASHAs are given a long notebook to maintain the records of 6- to 51-week-old children and 5- to 10-year-old children from their community. ASHAs regularly provide tablets to prevent anemia / credit: Sanket JainASHAs’ role doesn’t end with distributing medications. They answer questions people raise / credit: Sanket JainASHA Rani Koli, from Kolhapur’s flood-affected Bhendavade village, surveying her community after the July floods. “Even my house was ravaged by the 2019 and 2021 floods, but we keep working to make sure everyone remains safe,” she said / credit: Sanket JainASHA Kavita Patil talking to senior citizens in Kolhapur’s Bhendavade village to understand the mental toll of living through two floods / credit: Sanket JainASHA workers Netradipa Patil and Maya Patil surveying a community to learn more about how two floods and lockdowns affected the lives of rural community women / credit: Sanket Jain
Sanket Jain is an independent journalist based in the Kolhapur district of the western Indian state of Maharashtra. He was a 2019 People’s Archive of Rural India fellow, for which he documented vanishing art forms in the Indian countryside. He has written for Baffler, Progressive Magazine, Counterpunch, Byline Times, The National, Popula, Media Co-op, Indian Express and several other publications.